
How Many Steps Do You Really Need to Prevent Dementia?
The number 10,000 came from a 1960s Japanese pedometer ad. The number 9,826 came from a single observational study that can't prove what the headlines claim. Here's what the evidence actually supports

This is an occasional series looking at neuroscience beyond clinical trials - how we measure what we think we’re measuring, and what the data actually show. Brain Trials’ core coverage of neurodegeneration drug development continues next week.
You’ve seen the headlines. “Walking 9,800 Steps Daily Can Reduce Your Dementia Risk by 51%.” Or “Only 3,000 Steps a Day Cuts Alzheimer’s Risk by 25%.” Or “7,000 steps can cut health risks, including dementia”.


Some outlets went further: 10,000 steps is “the magic pill… better than any pill or injection currently available.” The claim is built on real studies, but the conclusion it’s not fully supported by the data.
And the number most people are chasing, 10,000 steps, was never based on science at all.
The number 10,000 is a marketing slogan
In 1965, the Yamasa Clock and Instrument Company released a pedometer called the Manpo-kei — Japanese for “10,000-step meter.” The name was chosen because the Japanese character for 10,000 (万) resembles a walking person, and because the number sounded aspirational. As Harvard epidemiologist I-Min Lee has noted, there were no studies behind it: 10,000 was round, memorable, and great for sales.1
Every modern study that frames its findings around 10,000 steps is, in effect, reverse-engineering a slogan. The number entered public health not through clinical evidence but through consumer electronics. It stayed there because nobody replaced it with anything better, until recently, when studies started trying to derive actual dose-response curves.
The results don’t land where most people expect.
The study behind the headlines
The most-cited evidence comes from del Pozo Cruz et al., published in JAMA Neurology in 2022.2 It analyzed 78,430 UK Biobank adults, aged 40–79, who wore a wrist accelerometer. Over a median follow-up of 6.9 years, 866 developed dementia: about 1.1% of the cohort.
Using spline-based Cox regression, they reported an “optimal” dose of 9,826 steps per day, associated with a 51% lower dementia risk (HR 0.49, 95% CI 0.39–0.62). A “minimal” dose of 3,826 steps was associated with a 25% reduction (HR 0.75, 95% CI 0.67–0.83). They also found that walking intensity mattered: a peak 30-minute cadence of 112 steps per minute was linked to a 62% lower risk, prompting an editorial titled “Is 112 the New 10,000?”
These numbers are precise, impressive, and, if you read closely, exactly the kind of false precision this newsletter was built to question.
What the study can’t tell you
If this analysis feels familiar, it should. The same UK Biobank, the same observational design, many of the same methodological blind spots. Readers of my recent sleep piece (May 2026) will recognize every one of these:

Reverse causality is the central threat. Dementia has a prodrome of a decade or more during which gait slows, motivation falls, and executive function declines. People who walk fewer steps may walk less because they are already developing dementia — not the other way around. This isn’t speculative. A landmark individual-participant meta-analysis of 19 cohorts found that when physical activity was measured more than 10 years before dementia onset, the association disappeared entirely (Kivimäki et al., BMJ 2019).3 Del Pozo Cruz’s median follow-up of 6.9 years sits squarely inside that prodromal window.
Healthy-volunteer bias. This is the same UK Biobank that recruited only 5.5% of those invited. Participants were less likely to smoke, less likely to be obese, and had mortality rates 46–56% lower than the general population (Fry et al., Am J Epidemiol 2017). The accelerometer sub-study is an even more selected slice. People who walk 10,000 steps in this cohort are systematically healthier in every dimension — diet, education, social engagement, cardiovascular fitness — making it nearly impossible to isolate the effect of steps from the effect of being the kind of person who walks 10,000 steps.
The “daily steps” measurement was a snapshot. Participants wore the accelerometer for roughly one week. “Daily steps” was calculated from as few as three valid days within that single window. This brief behavioral snapshot from 2013–2015 was then used to predict dementia outcomes years later, as if a 3-day accelerometer capture tells you how someone has been living for the previous decade, or will live for the next one.
The precision is false. Reporting an “optimal” dose of 9,826 steps (not 9,800, not “roughly 10,000”) implies a resolution the data cannot support. Wrist accelerometers are least accurate at exactly the slow walking speeds where older, at-risk populations live. Published validation studies show slow-walking step error can reach 24%, and consumer wearables over-count steps by 23–28% in free-living conditions versus research-grade devices.4 At that error margin, 3,826 steps and 5,000 steps are statistically indistinguishable from the same measurement.
The clinical trial evidence doesn’t match
Here is the part that almost never makes the headline: every randomized controlled trial of exercise for dementia prevention has been null or near-null.
The LIFE trial (JAMA 2015, n=1,635) randomized sedentary older adults to a 24-month structured walking and resistance program versus health education. No improvement in cognition. No reduction in dementia incidence.5
The DAPA trial (BMJ 2018, n=494) tested moderate-to-high-intensity exercise in people with mild-to-moderate dementia. Fitness improved. Cognitive decline was not slowed, and the exercise group was numerically worse on the primary cognitive measure.
The FINGER trial (Lancet 2015, n=1,260) is the only positive result, but exercise was bundled with diet, cognitive training, and vascular risk monitoring, making the walking contribution impossible to isolate. And the effect size was tiny (Cohen’s d ≈ 0.13).
This is the gap that matters. The observational data say “people who walk more get less dementia.” The trial data say “making people walk more doesn’t measurably prevent dementia.” Those two findings are not contradictory if the observational association is driven by reverse causality and confounding rather than by a causal effect of steps on the brain. That possibility is not a footnote. It is the most important caveat in the entire literature, and most coverage ignores it.
What the dose-response actually looks like
If the evidence doesn’t support 10,000, what number does hold up?
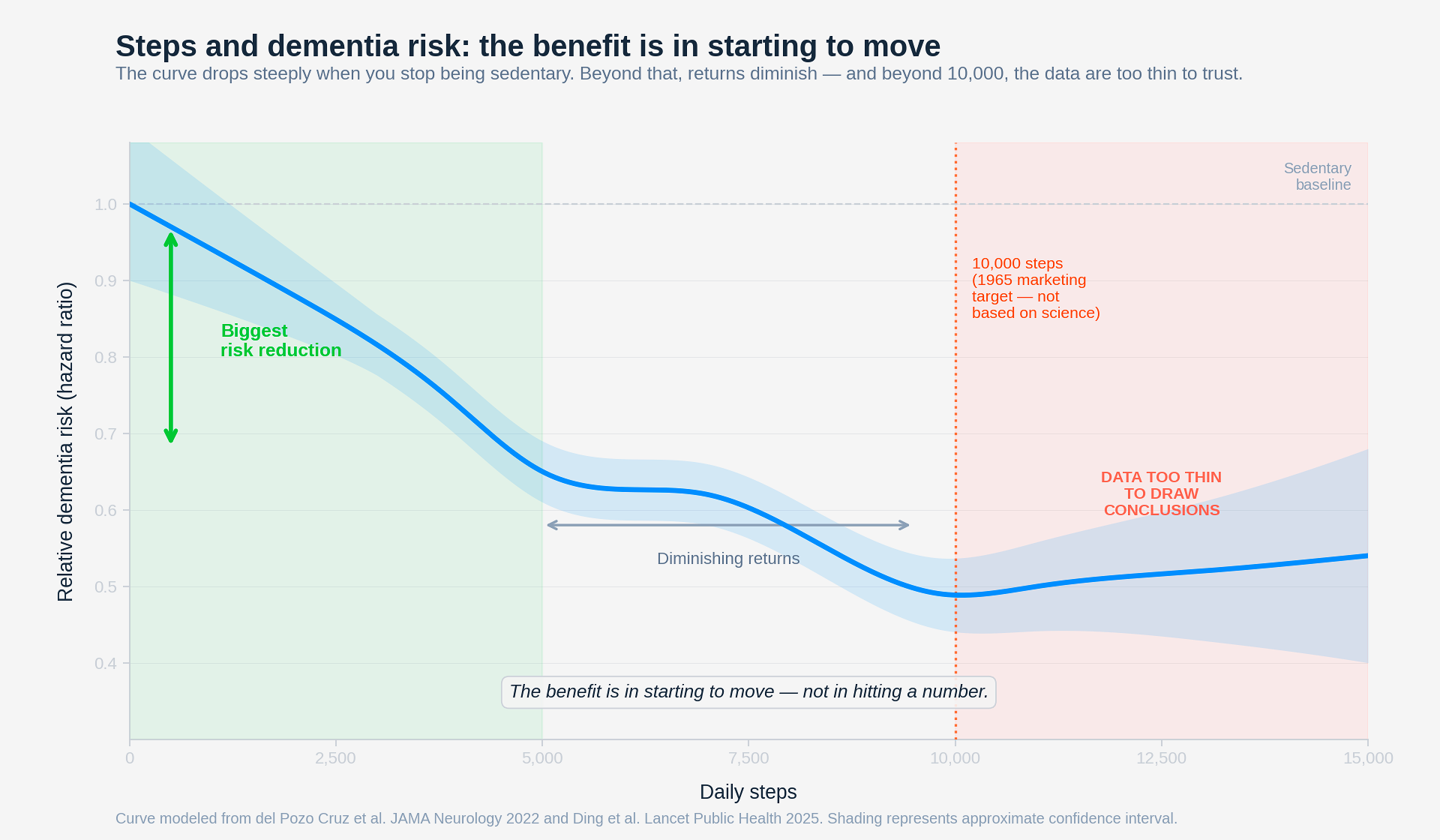
A 2025 dose-response meta-analysis in The Lancet Public Health (Ding et al., 57 studies, 35 cohorts) found the inflection point for dementia risk sat at roughly 5,000–7,000 steps per day, with a 38% lower risk at 7,000 versus 2,000 steps.6 A Nature Medicine study of the Harvard Aging Brain cohort found that the association between steps and slower tau accumulation plateaued at 5,001–7,500 steps.
The convergent signal across better-powered syntheses is that the largest marginal benefit comes from moving out of sedentary behavior, from near-zero to roughly 5,000 steps. Beyond 7,000, returns diminish. Beyond 10,000, the evidence is sparse and noisy.
So the real “optimal” isn’t a number. It’s a transition: from sitting to moving.
What you can honestly tell yourself
Walking is good for your brain. The biological plausibility is real: primarily through cardiovascular and metabolic health, which are genuine dementia risk factors supported by interventional evidence for those endpoints, even if not yet for dementia itself. The more recent tau-pathology finding is intriguing but observational.
But “how many steps prevent dementia” is a question the science cannot currently answer with a specific number. The observational data suggest more is better, with diminishing returns above 5,000–7,000. The clinical trial data have not confirmed that any specific step target prevents cognitive decline.
The honest claim, with the available data, is: physically active people appear to get less dementia. We have not proven that steps prevent dementia, and we have not identified a precise dose.
Walk because it’s good for your heart, your metabolism, your mood, and probably your brain. Don’t walk because your watch told you to hit a number that was invented to sell a pedometer in 1965, and don’t feel anxious if you fall short of a threshold that no randomized trial has validated.
Your body was designed to move through the day, not to hit a metric.
Just walk. Even if you don’t hit 10,000 or 7,000 steps.
I left out the wearable validation literature (which is a story in its own right and I will discuss in a future post), the question of whether walking intensity matters more than volume, and the striking new finding that steps may act on tau pathology but not on amyloid — which has implications for how the field designs prevention trials. Happy to go deeper on any of these if there’s interest. Let me know in a comment:
If this kind of analysis — the kind that reads the study behind the headline and tells you what it actually found — is useful to you, consider subscribing. Brain Trials looks critically at the science of the brain: the trials that shape treatment, the studies that shape understanding, and the claims that deserve a closer read.
The gap between what a study measures and what the headline claims it proves is where most health misinformation lives. Learning to see that gap is what clinical trial literacy is about. I wrote a book about that.
A Patient’s Guide to Clinical Trials: Navigating the Promise and Pitfalls of Experimental Treatments (Bloomsbury): available now.
Views expressed here are my own and not necessarily those of my employer.
References
del Pozo Cruz B, Ahmadi M, Naismith SL, Stamatakis E. Association of Daily Step Count and Intensity With Incident Dementia in 78,430 Adults Living in the UK. JAMA Neurology. 2022;79(10):1059–1063. doi:10.1001/jamaneurol.2022.2672
Kivimäki M, Singh-Manoux A, Pentti J, et al. Physical inactivity, cardiometabolic disease, and risk of dementia: an individual-participant meta-analysis. BMJ. 2019;365:l1495. doi:10.1136/bmj.l1495
Ding D, del Pozo Cruz B, Stamatakis E, et al. Daily steps and health outcomes in adults: a systematic review and dose-response meta-analysis. Lancet Public Health. 2025;10(7):e479–e490. doi:10.1016/S2468-2667(25)00108-0
Sink KM, Espeland MA, Castro CM, et al. Effect of a 24-Month Physical Activity Intervention vs Health Education on Cognitive Outcomes in Sedentary Older Adults: The LIFE Randomized Trial. JAMA.2015;314(8):781–790. doi:10.1001/jama.2015.9617
Fry A, Littlejohns TJ, Sudlow C, et al. Comparison of Sociodemographic and Health-Related Characteristics of UK Biobank Participants With Those of the General Population. American Journal of Epidemiology.2017;186(9):1026–1034. doi:10.1093/aje/kwx246
Feehan LM, Geldman J, Sayre EC, et al. Accuracy of Fitbit Devices: Systematic Review and Narrative Syntheses of Quantitative Data. JMIR mHealth uHealth. 2018;6(8):e10527. doi:10.2196/10527
Ngandu T, Lehtisalo J, Solomon A, et al. A 2 year multidomain intervention of
diet, exercise, cognitive training, and vascular risk monitoring versus control
to prevent cognitive decline in at-risk elderly people (FINGER): a randomised
controlled trial. Lancet. 2015 Jun 6;385(9984):2255-63. doi:
Footnotes
The Manpo-kei pedometer was developed by engineer Juri Kato at Yamasa Clock and Instrument Company after Tokyo physician Iwao Ohya recommended 10,000 daily steps to counter sedentary habits ahead of the 1964 Olympics. No clinical trial or epidemiological study supported the number. Harvard epidemiologist I-Min Lee confirmed to Popular Science: “There were no actual studies that had looked at ‘10,000 steps’… It was a made-up number in the sense that 10,000 sounds good, it’s easy to remember.”
del Pozo Cruz B, Ahmadi M, Naismith SL, Stamatakis E. Association of Daily Step Count and Intensity With Incident Dementia in 78,430 Adults Living in the UK. JAMA Neurology. 2022;79(10):1059–1063. 78,430 UK Biobank adults, Axivity AX3 wrist accelerometer, median 6.9-year follow-up, 866 dementia events. The “optimal” 9,826 and “minimal” 3,826 step thresholds are model-derived inflection points from restricted cubic spline Cox regression, not pre-specified clinical thresholds.
Kivimäki M, Singh-Manoux A, Pentti J, et al. Physical inactivity, cardiometabolic disease, and risk of dementia: an individual-participant meta-analysis. BMJ. 2019;365:l1495. 404,840 participants from 19 cohorts. The key finding: physical inactivity was associated with dementia only when measured within 10 years of diagnosis. With longer intervals, the association vanished — consistent with reverse causation (prodromal dementia → reduced activity, not the reverse).
Feehan LM et al. Accuracy of Fitbit Devices: Systematic Review and Narrative Syntheses of Quantitative Data. JMIR mHealth uHealth. 2018;6(8):e10527. Reviewed 67 studies. Fitbit met acceptable step-count accuracy about half the time, with systematic overestimation in free-living settings. Slow-walking error can reach ~24% mean absolute percentage error.
Sink KM, Espeland MA, Castro CM, et al. Effect of a 24-Month Physical Activity Intervention vs Health Education on Cognitive Outcomes in Sedentary Older Adults: The LIFE Randomized Trial. JAMA.2015;314(8):781–790. The largest and longest exercise-only RCT for cognitive outcomes in older adults. 1,635 sedentary adults aged 70–89, randomized to structured moderate-intensity walking + resistance training versus health education. No significant between-group differences on any cognitive measure.
Ding D, del Pozo Cruz B, Stamatakis E, et al. Daily steps and health outcomes in adults: a systematic review and dose-response meta-analysis. Lancet Public Health. 2025;10(7):e479–e490. The dementia-specific estimate is based on 2 studies, yielding HR 0.62 (95% CI 0.53–0.73) for 7,000 vs 2,000 steps — but the thinness of the pooled evidence base deserves caution despite the confident-sounding number.
Jose-Alberto, the question your piece raises by accident is why the number keeps outliving its own evidence. I think it is because the number was never really doing evidential work. It was doing emotional work.
Dementia is the worst kind of fear to sit with, slow and impossible to picture in advance. A step target converts that into something you can finish by bedtime, and the watch hands you a verdict every night. Swapping 10,000 for 7,000 changes nothing that matters, because the problem was never the figure but the promise it is asked to carry: protection from a future no trial has shown walking can buy. The count becomes a receipt for something the evidence has not sold.