
Why We Faint
The first time I fainted, I was a medical student dissecting a vagus nerve. What happened in my body that day was older than humans — and it had nothing to do with me being weak.

A neuroscience piece this slow summer week — about the autonomic nervous system, evolution, and the reflex that drops healthy people to the floor. Clinical trials return next week with the AAIC 2026 preview. If you're new here: Brain Trials covers both the science of neurological disease and the trials that shape how it's treated.
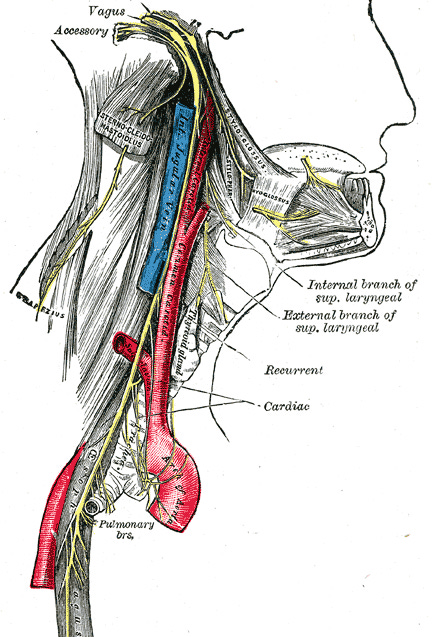
I was twenty years old. Second year of medical school. We were in the physiology lab, six of us around a stainless steel table, and the assignment that afternoon was the autonomic nervous system. What we needed to expose was the vagus nerve — the long, wandering nerve that runs from the brainstem down into the chest and abdomen, the body’s primary brake on the heart.
I made the incision. I remember the smell first. Warm blood has a particular smell — metallic, slightly sweet, the iron in hemoglobin reacting with the air. It got warmer as I leaned in. My hands were steady. I started looking for the nerve.
And then, in the order they always come: my palms went wet, my face went pale, my vision narrowed at the edges, and somewhere in my chest I felt the strange certainty that something was about to happen that I could not stop.
I do not remember hitting the floor.
What I remember next is voices. Then vision, returning in pieces. Then a wave of nausea so complete it felt like the world tilting. My classmates were standing over me, holding my head up, telling me I was fine. I did not feel fine. I felt poisoned.
I had fainted. Cleanly, classically, textbook. And I had done it while literally dissecting the nerve responsible for the reflex that had just dropped me to the floor.
It would take me years — through medical school, residency, a fellowship in autonomic disorders, and thousands of patients — to fully understand what had happened to my body that afternoon. The short version is this: there was nothing wrong with me. The reflex worked perfectly. The problem was that the reflex was designed for a world I no longer lived in.
What was happening inside me
A vasovagal faint unfolds in two phases.
The first is mobilization. Something — a sight, a smell, the anticipation of pain, the sensation of warm blood under your fingers — triggers a surge of sympathetic activity. Heart rate climbs. Blood pressure rises. Adrenaline floods the system. The palms go wet because sweat improves grip, and grip used to matter. The skin goes pale because blood is being redirected from the surface to the muscles. The mouth goes dry. This is the body’s standard threat response, the one we share with every vertebrate that has ever needed to run from something.
The second phase is the strange one. If the threat does not resolve — if the stimulus continues, if there is no escape — the autonomic system does something counterintuitive. It throws the brake. Hard. The vagus nerve, which normally exerts a moderate, continuous restraint on the heart, fires with such force that the heart rate plunges. Blood vessels in the legs and abdomen dilate, dropping blood pressure further. Within seconds, the brain — perched at the top of a five-foot column of fluid that suddenly has nothing pushing it upward — runs out of blood.
You lose consciousness. You fall. Your body, no longer fighting gravity, becomes horizontal. Blood returns to the brain. You wake up.
Then, because the autonomic system has just emptied a massive surge of vasopressin into your bloodstream — a hormone that helps restore blood pressure but happens, as a side effect, to cause profound nausea — you feel terrible for the next half hour. In a 2020 New England Journal of Medicine review I wrote with my mentor Horacio Kaufmann and our colleague Lucy Norcliffe-Kaufmann, we documented this neurohormonal cascade in sixty-three patients with vasovagal syncope.1 The vasopressin spike at the moment of fainting is the body trying to restore its pressure. The nausea that follows is the price.
That’s what happened to me on the floor of the anatomy lab. Surrounded by classmates who, like all medical students before them, had been warned that this would happen to someone in the room and were just relieved it wasn’t them.
Why this reflex exists at all
Here’s the question that took me years to think clearly about. If fainting is so functionally useless — dropping unconscious in front of a predator, in the middle of a hunt, on the side of a road — why has evolution kept it? Why does every healthy human carry, in their wiring, a reflex that can incapacitate them at the worst possible moment?
The answer, proposed by the Italian cardiologist Paolo Alboni and developed across a series of papers over the past two decades, is that the vasovagal reflex isn’t a malfunction at all. It is a passive defense response that worked beautifully for half a billion years — until the conditions under which it worked stopped existing.
The closest analog in other mammals is something called tonic immobility — the technical term for “playing dead.” When an opossum is caught by a predator, it does not fight. It collapses. Its body goes stiff. Its heart rate plummets. Its breathing slows. And — for full theatrical effect — its anal glands secrete a foul-smelling green liquid that mimics decomposition. Predators, which are generally adapted to detect and pursue moving prey, frequently lose interest. Many release their grip. The opossum lies still until the threat passes, then gets up and walks away.
This is the same circuitry, biologically, that drops a medical student onto an anatomy lab floor. Heart rate crashes. Blood pressure crashes. Movement ceases. The animal looks dead.
In the opossum, consciousness is preserved during this — the animal is paralyzed but aware, watching for its moment. In humans, the reflex evolved to cause loss of consciousness, probably as a side effect of two specifically human adaptations: an upright posture that puts the brain much higher above the heart than in a quadruped, and a large brain that requires constant high blood flow. When the vasovagal reflex fires hard in a creature standing on two legs with a hungry cortex on top, you don’t go limp watching for an opening. You go down.
The reflex still works. The trigger has changed. Predators used to be the trigger. Now it’s the sight of blood, a needle, a hot crowded room, the anticipation of bad news, or — for a generation of medical students — the lab assignment in which they are required to lean over a body and cut into the very nerve that is about to take them out.
Why we are uniquely vulnerable
There is a second, separate problem with fainting that has nothing to do with predator defense. It has to do with the fact that humans are, in evolutionary terms, very recently and very awkwardly upright.
When you stand up, blood pools briefly in your legs. Your autonomic system has to detect the drop and restore pressure to your brain within seconds. If any link in that chain delays, you feel lightheaded. If it fails outright, you faint.
Humans are uniquely vulnerable to this. Our nearest primate relatives, when they assume an upright posture, have shorter distances between heart and brain and less blood pooling in the lower body. They almost never faint orthostatically. And then there’s the giraffe, which solved the upright-circulation problem with such elegance that physiologists have spent decades studying it: blood pressure roughly twice ours, a heart that weighs over twenty pounds, and skin so tight it functions like compression stockings. A giraffe lifting its head from a drink at ground level experiences a pressure change that would drop a human instantly. It walks away.
We did not solve the problem. We just got mostly good enough.
Which is why, every summer in London, photographs circulate of Royal Guards collapsing in front of Buckingham Palace, falling sideways in their bearskin hats while the crowd takes pictures. The internet treats this as something funny or scandalous. It is neither. It is what happens when a healthy young human stands motionless in hot wool in direct sun for hours, gradually loses fluid, develops mild dehydration, and asks an autonomic system designed for hunting and gathering to maintain cerebral perfusion through conditions it was never built to handle. The Guards are not weak. They are not poorly trained. They are running healthy autonomic systems in deeply unnatural conditions, and the system is doing the only thing it can.
This is the running theme. The reflex is fine. The world is the problem.
What I tell patients
When a patient comes to my clinic having fainted, the first thing I do — before any test, before any imaging, before any discussion of treatment — is ask them to tell me exactly what they were doing in the minutes before they lost consciousness. What did they see? What did they smell? What did they feel? Were they standing? For how long? Had they eaten? Had they been drinking water?
Most of the time, by the end of the story, both of us can already tell what happened. The body is honest about these things. It leaves a trail.
What I also try to say, before the workup begins, is what the body was actually doing. Not because it changes the management — sometimes it does, sometimes it doesn’t — but because most people who faint have spent the time between the event and the appointment afraid that something is fundamentally wrong with them. They are imagining their hearts failing, their brains breaking, their bodies rebelling against them in some way they cannot understand.
Almost always, they are wrong about that.
The reflex that drops a medical student to a tile floor in an anatomy lab is the same reflex that drops a soldier in a hot uniform, a witness at a wedding, a pharma executive near the President of the United States, a parent in the labor room watching his first child being born. It is the same reflex that, in a different form, lets an opossum walk away from a coyote. It is half a billion years old. It works.
The world it works in is the one we no longer live in. You are not broken. The reflex is fine. The fit between the two is what has shifted, and that fit is what most people experiencing strange bodily events are actually contending with.
This is what I have come to think most of medicine, at the level of the autonomic system, is really about. Not fixing wiring that has gone wrong. Translating, for people who have been told they are broken, what an old and intelligent system was actually trying to do in conditions it was never built to face. Most of what arrives in an autonomic clinic is some version of this — a body running an ancient program faithfully, in a world that no longer matches the program.
The lab assignment, that afternoon, was to find the vagus nerve. I found it. It introduced itself.
A note on what this piece does not cover: there are forms of fainting that are not vasovagal, and some of them are dangerous. Cardiac arrhythmias, severe orthostatic hypotension in the context of autonomic failure that accompanies certain neurodegenerative diseases like Parkinson’s, all produce loss of consciousness that requires medical evaluation. If you’ve fainted without a clear trigger, fainted during exertion, or developed a pattern of lightheadedness on standing, particularly later in life, see a doctor. I’ll write more about when to worry in a future piece, if there is interest (leave a comment to let me know).
If this kind of writing interests you — the place where evolution, neuroscience, and the body’s hidden architecture meet — this is the territory I’ll be exploring more on Brain Trials over the coming months.
Further reading
Alboni P, Alboni M, Bertorelle G. The origin of vasovagal syncope: to protect the heart or to escape predation? Clinical Autonomic Research, 2008.
Alboni P, Alboni M. Vasovagal syncope as a manifestation of an evolutionary selected trait. Journal of Atrial Fibrillation, 2014.
Kaufmann H, Norcliffe-Kaufmann L, Palma JA. Baroreflex Dysfunction. N Engl J Med 2020;382:163-178.
Mitchell G, Skinner JD. An allometric analysis of the giraffe cardiovascular system. Comparative Biochemistry and Physiology, 2009.
Footnotes
Kaufmann H, Norcliffe-Kaufmann L, Palma JA. Baroreflex Dysfunction. New England Journal of Medicine. 2020;382(2):163-178. doi:10.1056/NEJMra1509723. The neurohormonal cascade during vasovagal syncope, including the plasma vasopressin spike at the moment of consciousness loss, is documented in Figure 2C of this review (n=63 patients).